The Event
- PIA 8303 approaches Karachi on a scheduled service from Lahore
- From at least 10 nautical miles, the approach is above profile and above speed — unstabilised
- The crew do not conduct a stabilised approach check; descent continues
- On final approach, ATC transmits that the gear appears not extended
- The landing gear warning horn activates as the aircraft descends through the gear-down altitude
- The crew acknowledge the warning and continue the approach without lowering the gear
- The aircraft touches down on both engine nacelles at approximately 180 knots — both engines contact the runway
- The crew execute a go-around; on the second approach both engines fail from nacelle damage
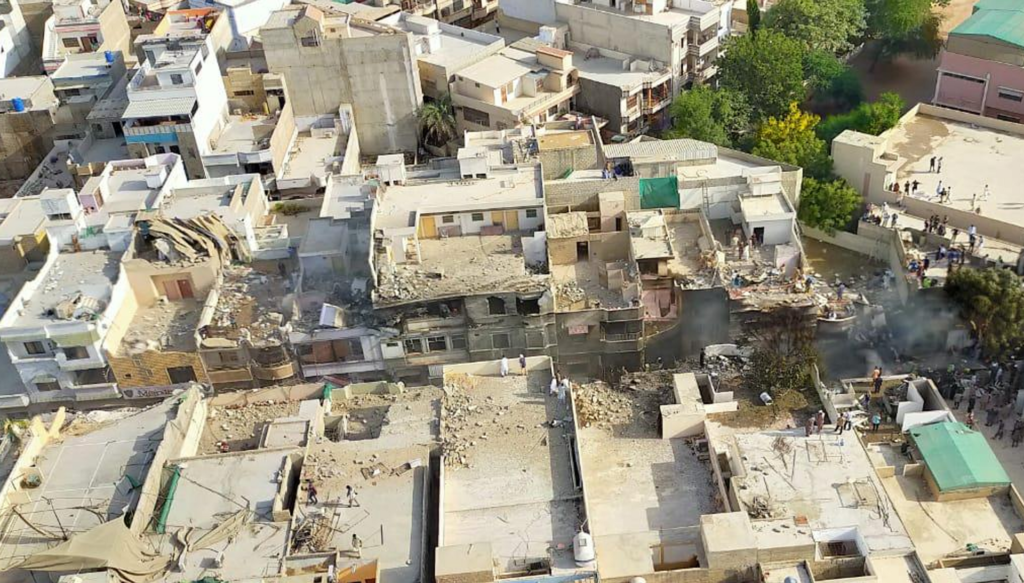
- The aircraft impacts the Model Colony residential area short of the runway
- 97 of 99 on board die; 1 person on the ground dies
The investigation found that CVR recordings contained extensive evidence of mobile phone use by both crew members during the approach. Investigation by Pakistan’s government also found that 262 of Pakistan’s commercial pilots held fraudulent or inadequately-documented licences — a systemic regulatory failure that contributed to EU suspension of PIA’s operating rights.
Systems Engineering Perspective
From a systems engineering perspective, PIA 8303 is a safety management system failure at every level simultaneously: crew discipline, organisational safety culture, operator safety management, and regulatory oversight. It is the case study that shows what aviation looks like when the safety system has effectively stopped working.
PIA 8303 is not a case where the safety system encountered an unusual challenge and failed. It is a case where the safety system had stopped functioning before this flight ever departed. The accident was the visible outcome of an invisible systemic collapse.
The Gear Warning System — Working Correctly, Actioned Incorrectly
The A320 gear warning horn activates at defined altitudes when the landing gear is not selected down. The system worked correctly on PIA 8303 — it provided the correct warning at the correct time. The crew acknowledged the warning. They continued the approach without lowering the gear.
This is the safety system’s most fundamental failure mode: the protection worked, the warning was heard, and the action required was not taken. No engineering solution can protect against a crew that acknowledges a warning and chooses not to act on it.
A safety warning that is heard and not actioned is no longer a safety barrier. The protection exists only if the required action follows the warning. PIA 8303 demonstrated that the action can be absent even when the warning is present.
Mobile Phone Use During Approach
The CVR captured mobile phone use by both crew members during the final phase of the approach — a phase that was already unstabilised, already in IMC, and already producing ATC warnings about gear position. The cognitive resources required for phone use were directly competing with the resources required for approach monitoring.
This is not a unique incident in PIA operations. The investigation found evidence that mobile phone use during approach was normalised behaviour across the operation — not an isolated crew aberration but a cultural norm that the safety management system had not identified or addressed.
Human Factors Perspective
The human factors analysis operates at the systemic level. The crew-level errors are documented and clear. The systemic questions are: how does a safety management system produce this level of normalised non-compliance, and what does it require to rebuild?
Normalised Non-Compliance
Mobile phone use during approach, unstabilised approaches continued past the gate, gear warnings not actioned — these are not isolated failures. They are behaviours that become normalised in an operational culture where the safety management system is not functioning to identify, address, and correct them. Normalised non-compliance does not happen overnight. It builds over years of non-enforcement, creating a culture where the gap between procedure and practice feels normal.
Normalised non-compliance is the most dangerous safety system condition. It is invisible from inside the culture that produces it. Its detection requires external audit, objective data analysis, and leadership that treats the gap between procedure and practice as a safety emergency.
Regulatory Collapse — Fraudulent Licences
The investigation into PIA 8303 triggered a broader audit of Pakistani commercial pilot licences that found 262 pilots holding fraudulent or inadequately-documented licences. This finding — that a significant fraction of the commercial pilot population had not been properly qualified — represents a regulatory oversight failure that is, in scale and implication, among the most serious in civil aviation history.
System Interaction Breakdown
1. Unstabilised Approach Continued Past Gate
The approach was high and fast throughout. The stabilised approach standard was not applied.
2. Gear Warning Not Actioned
The gear warning horn activated. ATC transmitted gear warnings. The crew acknowledged and continued.
3. Mobile Phone Use During Critical Phase
Both crew were using mobile phones during the final approach phase — reducing cognitive resource available for approach monitoring.
4. Second Approach Flown With Damaged Engines
The go-around was executed with engine nacelles damaged by runway contact on the first touchdown. Both engines failed on the second approach.
Significance in Aviation Risk
1. ICAO Significant Safety Concern — Pakistan
Pakistan’s Civil Aviation Authority was placed on ICAO’s Significant Safety Concern list.
2. EU Suspension of PIA Operating Rights
The European Union Aviation Safety Agency suspended PIA’s rights to operate to European destinations pending safety improvements.
3. Pakistani Licence Audit
The licence audit that followed found 262 fraudulently-documented licences — triggering an international suspension of those licence holders.
4. PIA Safety Programme Restructuring
PIA undertook a significant safety management programme restructuring with international support — a process that mirrors, at smaller scale, the Korean Air transformation after 1999.
Related Aviation Risk Lab Content
Pillar Pages
Human Factors: Human Factors
Safety Engineering: Safety Engineering
Crew Resource Management: Crew Resource Management
Related Case Studies
Case Study 11: Korean Air 801 — CFIT, Authority Gradient: Korean Air 801
Case Study 22: Germanwings 9525 — The System That Couldn’t See: Germanwings 9525
Case Study 29: Air France 296 — The Air Show and the Trees: Af 296
Closing Perspective
PIA 8303 is the most extreme example in this library of what happens when a safety management system stops working. It is not the story of a crew making errors under pressure. It is the story of an organisation that had normalised non-compliance to the point where a gear warning horn on final approach was not sufficient to produce the action required.
Korean Air’s transformation after 1999 shows that an airline can rebuild its safety culture from the ground up. PIA’s post-2020 reform process is attempting the same. The difference is that Korean Air did it after fatal accidents in the late 1990s. PIA began after a fatal accident in 2020. The process is the same. The cost of starting late is the same.
Safety culture is not inherited. It is built. PIA 8303 is the price of not building it fast enough.
PIA 8303 is the case study that shows what aviation looks like when the safety management system has stopped working. The gear warning worked. The crew did not. The system behind them had not worked for a very long time.


")






