The Event
- Flight 173 approaches Portland; a gear extension produces an abnormal noise and an uncertain indicator
- Captain initiates holding pattern at 2,000 feet over eastern Portland suburbs to troubleshoot
- Gear is in fact down and locked — the indication was spurious, but the crew cannot confirm this
- Over the next 68 minutes the captain works through checklists with the crew
- The flight engineer makes multiple references to the diminishing fuel state
- At 17:46, with approximately 5,000 lb remaining — below minimum safe quantity — the captain acknowledges the concern but continues holding
- Engines begin to flame out from fuel starvation
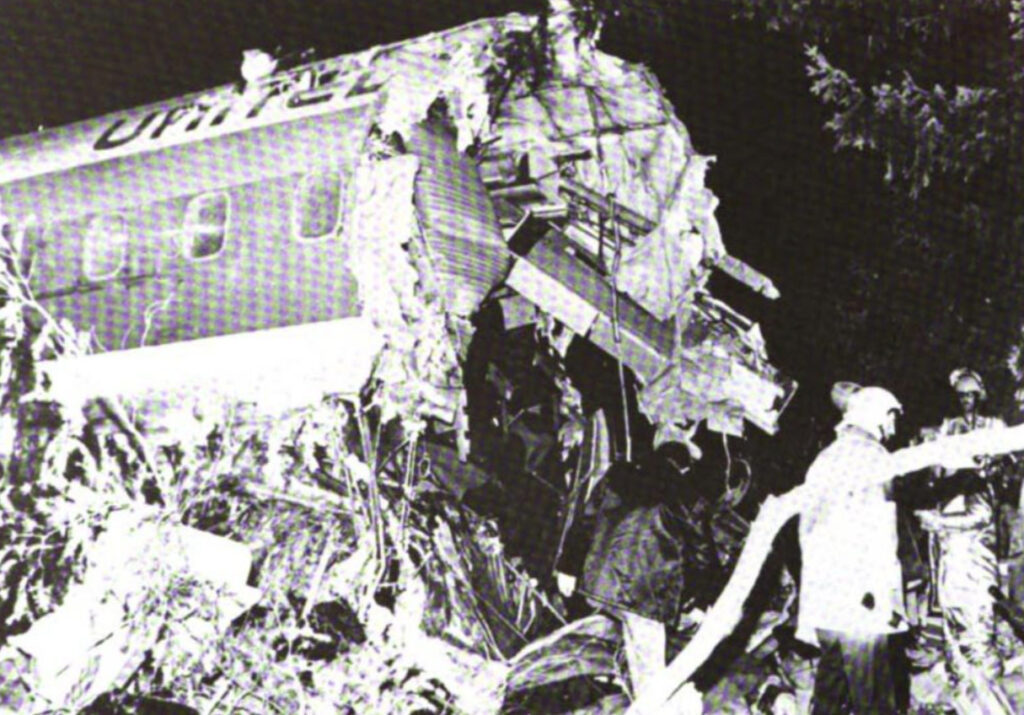
- Flight 173 strikes trees 6 nautical miles short of Portland International Airport
- 10 people die; 179 survive — the aircraft was still technically flyable when the decision to land could have been made
An NTSB investigator later described United 173 as the accident that proved Tenerife’s lesson applied inside the cockpit — not just between cockpits.
Systems Engineering Perspective
From a systems engineering perspective, United 173 exposes a critical gap in the fuel management oversight architecture of commercial transport operations in 1978. The DC-8’s fuel system was working correctly throughout. The instrumentation provided accurate, real-time fuel state data. The system failure was not in the fuel or its measurement — it was in the decision-making and communication architecture that surrounded that data.
A system that generates accurate safety-critical data but has no mechanism to ensure that data reaches a decision is not a safe system. The data must be actionable.
Absence of a Fuel Emergency Threshold
The DC-8’s procedures did not define an explicit fuel state at which the captain was required to take action — no mandatory go/no-go decision gate, no hard lower limit below which holding was procedurally prohibited. The decision to continue holding, or to initiate an approach, was left entirely to the captain’s judgment.
In a system where the authority of the captain is absolute, the absence of a procedural forcing function means that the captain’s personal judgment — whatever its quality — cannot be overridden by any technical or procedural mechanism. United 173 demonstrated that personal judgment, under the right conditions of fatigue, tunnel focus, and authority, can be catastrophically wrong.
Without a procedural or technical forcing function, fuel management becomes entirely captain-dependent. United 173 showed what happens when that dependency is the only layer of defence.
Indirect Communication as a System Failure Mode
The first officer and flight engineer communicated the fuel concern using indirect language: ‘We’re running low on fuel,’ ‘Getting a little low on fuel,’ ‘We have roughly four thousand pounds of fuel.’ Each statement was factually correct. None constituted an unambiguous demand for immediate action.
This indirectness was not accidental. It was culturally appropriate. In 1978, direct challenge of a captain’s decision by a junior officer was professionally risky and socially impermissible. The crew expressed concern in the only way the cultural system allowed — obliquely, deferentially, carefully. The captain heard data points. He did not hear emergencies.
In a system where direct challenge is culturally forbidden, indirect warnings are the only available communication tool. And indirect warnings can be — and are — missed.
No Low-Fuel Technical Alert Requiring Captain Action
There was no low-fuel alert on the DC-8 that the captain could not suppress or defer. No system in the cockpit escalated the fuel state to a mandatory decision trigger independent of the captain’s judgment. The entire safety architecture for fuel management rested on a single mechanism: the captain deciding to act.
A single-layer, single-actor safety system is not a system with safety. It is a system with a hope.
Human Factors Perspective
United 173 is the accident that gave CRM its name and purpose. The human factors analysis centres on the concept of captainitis — the first officer’s psychological and professional inability to directly challenge the captain’s authority — and on the transformation this accident triggered in aviation’s understanding of flight deck culture as a safety system.
Captainitis — The Named Phenomenon
The term ‘captainitis’ was coined in part to describe what happened aboard UAL 173. The captain was experienced, competent, and thoroughly absorbed in a genuine technical problem. The first officer and flight engineer possessed the information that would have saved the aircraft. Neither possessed the culturally-sanctioned authority to deliver it in a form that the captain was required to act upon.
This is not a story about a bad captain. It is a story about a cultural system that had encoded authority into silence — where the only person with the authority to act was the person least able, in that moment, to perceive the need to act.
Captainitis is not a personality defect. It is a predictable outcome of any hierarchical system where challenge carries professional risk.
Assertion Without Consequence
The crew asserted. Their assertions were heard. They produced no action. This is the moment where the concept of graduated assertion — assert, escalate, physically intervene — became necessary. Without a framework that requires the captain to respond to a stated safety concern, and that empowers the first officer to escalate if no response is forthcoming, the assertion is performative rather than functional.
United 173 demonstrated that training crew members to communicate safety concerns is insufficient if the captain is not equally trained to receive, acknowledge, and respond to them as obligatory safety inputs.
The Foundation of Modern CRM
United Airlines, working with psychologist Robert Helmreich and building on the NASA workshop findings that Tenerife had catalysed, developed the world’s first formal Crew Resource Management training programme directly as a response to UAL 173. The programme reframed the flight deck not as a hierarchy with one decision-maker and supporting staff, but as a team system in which every member has an equal safety responsibility and an equal obligation to assert and respond to safety concerns.
CRM is now mandated by every major regulatory authority on earth. United 173 is the reason.
System Interaction Breakdown
1. Single Decision-Maker Architecture
The captain was the only person who could order a landing. He was also the person most cognitively committed to the troubleshooting task. The system had no mechanism to require him to attend to fuel state at a minimum interval, no procedure that said ‘below X fuel, the approach must commence,’ and no co-pilot with the empowered authority to initiate one.
A safety system with a single human decision-maker and no procedural forcing function is not redundant. It is singular.
2. Information Available But Not Actionable
The fuel data was accurate, visible, and repeatedly vocalised. It was not actionable because the communication system — the cultural norms of the cockpit — did not provide a channel through which junior crew data could become captain action without the captain’s own initiative. Information that cannot reach decision-makers in actionable form is, from a systems perspective, as useful as information that does not exist.
3. Troubleshooting Without Time-Boundary
The troubleshooting process had no procedural time limit. There was no checklist item that said ‘if gear status unresolved after X minutes, land on the best available information.’ The captain could hold indefinitely. In the absence of a structural boundary, time — and fuel — continued to run.
Troubleshooting without a time boundary, combined with a fuel-finite aircraft, is a failure mode that requires no additional triggers to become fatal.
Significance in Aviation Risk
1. CRM — The Most Important Safety Programme in Aviation History
No single training programme has saved more lives in aviation than CRM. Its mandating across commercial aviation, military aviation, and progressively into maintenance and ATC, is a direct legacy of United 173.
2. The Assert-Escalate-Override Framework
Modern CRM training includes explicit, rehearsed protocols for asserting safety concerns, escalating when not actioned, and — in extremis — physically preventing a hazardous action. This graduated intervention framework was born from the UAL 173 crew’s inability to translate correct information into corrective action.
3. Fuel Emergency Thresholds
Airlines revised their operating procedures to define explicit minimum fuel states requiring immediate approach initiation, independent of troubleshooting status. These are now hard limits in SOPs, not discretionary guidelines.
Related Aviation Risk Lab Content
Pillar Pages
Crew Resource Management: Crew Resource Management
Human Factors: Human Factors
Safety Engineering: Safety Engineering
Related Case Studies
Case Study 1: Tenerife — When a System Has No More Margins Left: Tenerife 1977
Case Study 2: Eastern 401 — The Altitude No One Owned: Eastern 401
Case Study 18: Avianca 052 — Fuel, Holding and the Language Barrier: Avianca 052
Closing Perspective
United 173 is the case study that broke the myth of the all-knowing captain. It demonstrated, with ten fatalities and 179 near-misses, that placing sole decision-making authority in one person without any mechanism for challenge, constraint, or override is not a safety system — it is a single point of failure in human form.
The first officer on United 173 knew the aircraft was going to run out of fuel. So did the flight engineer. The system they were operating in had no way to translate their knowledge into the captain’s action. That gap was the accident.
CRM closed that gap. It remains the most important ongoing legacy of United 173 — a programme that has prevented thousands of accidents by giving every crew member not just permission, but an explicit professional obligation, to speak up.
United 173 proved that safety is not the captain’s job. Safety is the crew’s job. CRM is the system that makes that principle operational.

")

")